 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Aortic Stenosis
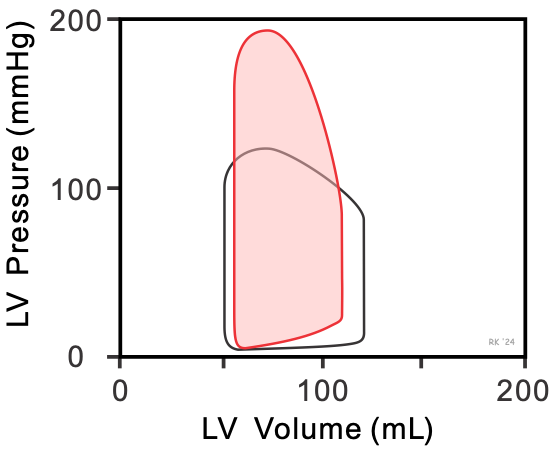 The following describes changes that may occur in the left ventricular pressure-volume (PV) loop in the presence of chronic aortic stenosis. In aortic stenosis (red loop in figure), left ventricular emptying is impaired because of high outflow resistance caused by a reduction in the valve orifice area when it opens. This high outflow resistance causes a large pressure gradient to occur across the aortic valve during ejection, such that the peak systolic pressure within the ventricle is increased. This leads to an increase in ventricular wall stress (afterload), a decrease in stroke volume (width of PV loop), and an increase in end-systolic volume compared to normal (black loop). Stroke volume decreases because the velocity of fiber shortening is decreased by the increased afterload (see force-velocity relationship). Despite the elevated end-systolic volume, the end-diastolic volume usually decreases because, over time (years, decades), the ventricle wall becomes thicker (hypertrophied). This increases ventricular stiffness (decreases compliance), which causes a large elevation in end-diastolic pressure despite reduced filling. Although the stroke volume is reduced, the end-diastolic volume is also reduced and therefore the ejection fraction does not decrease significantly. This represents a condition of heart failure with preserved ejection fraction (HFpEF), or diastolic dysfunction.
The following describes changes that may occur in the left ventricular pressure-volume (PV) loop in the presence of chronic aortic stenosis. In aortic stenosis (red loop in figure), left ventricular emptying is impaired because of high outflow resistance caused by a reduction in the valve orifice area when it opens. This high outflow resistance causes a large pressure gradient to occur across the aortic valve during ejection, such that the peak systolic pressure within the ventricle is increased. This leads to an increase in ventricular wall stress (afterload), a decrease in stroke volume (width of PV loop), and an increase in end-systolic volume compared to normal (black loop). Stroke volume decreases because the velocity of fiber shortening is decreased by the increased afterload (see force-velocity relationship). Despite the elevated end-systolic volume, the end-diastolic volume usually decreases because, over time (years, decades), the ventricle wall becomes thicker (hypertrophied). This increases ventricular stiffness (decreases compliance), which causes a large elevation in end-diastolic pressure despite reduced filling. Although the stroke volume is reduced, the end-diastolic volume is also reduced and therefore the ejection fraction does not decrease significantly. This represents a condition of heart failure with preserved ejection fraction (HFpEF), or diastolic dysfunction.
The fall in stroke volume can lead to a reduction in arterial pressure. Over time, the stroke volume may fall even further as the ventricle exhibits systolic and diastolic dysfunction. Compensatory increases in end-diastolic volume resulting from compensatory increases in blood volume and cardiac filling pressures will be limited by stiffened ventricular.
Revised 02/03/2024