 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Mitral Regurgitation
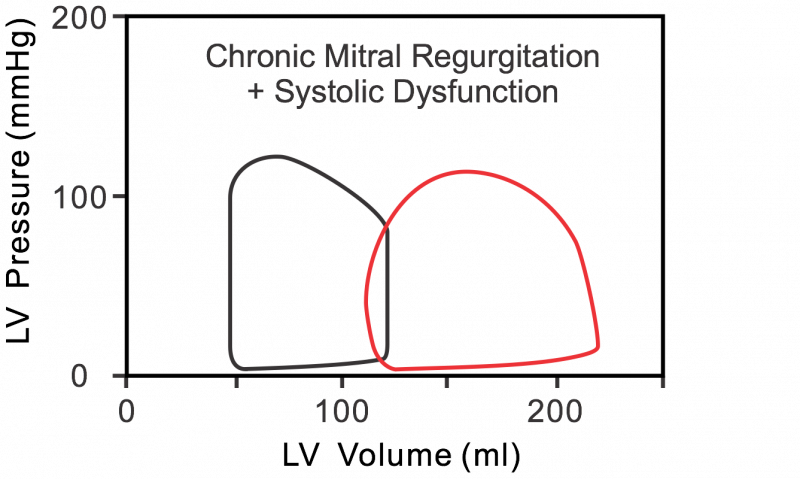 The following describes changes that occur in the left ventricular pressure-volume loop when there is chronic mitral regurgitation. In mitral valve regurgitation (red loop in figure), as the left ventricle contracts, blood is not only ejected into the aorta but also back into the left atrium. This causes left atrial volume and pressure to increase abnormally during ventricular systole. Note in the pressure-volume loop that there is no true isovolumetric contraction phase (no vertical line between mitral valve closure and aortic valve opening) because blood flows across the mitral valve and back into the atrium as soon as ventricular pressure exceeds left atrial pressure. Regurgitation continues after aortic valve opening. The net effect is that the ventricular stroke volume (EDV-ESV; width of loop) is increased.
The following describes changes that occur in the left ventricular pressure-volume loop when there is chronic mitral regurgitation. In mitral valve regurgitation (red loop in figure), as the left ventricle contracts, blood is not only ejected into the aorta but also back into the left atrium. This causes left atrial volume and pressure to increase abnormally during ventricular systole. Note in the pressure-volume loop that there is no true isovolumetric contraction phase (no vertical line between mitral valve closure and aortic valve opening) because blood flows across the mitral valve and back into the atrium as soon as ventricular pressure exceeds left atrial pressure. Regurgitation continues after aortic valve opening. The net effect is that the ventricular stroke volume (EDV-ESV; width of loop) is increased.
There is no true isovolumetric relaxation (vertical lines between aortic valve closure and mitral valve opening) because when the aortic valve closes and the ventricle begins to relax, the mitral valve is not completely closed, so blood continues to flow back into the left atrium (therefore further decreasing ventricular volume) as long as intraventricular pressure is greater than left atrial pressure. During ventricular diastolic filling, the elevated pressure within the left atrium is transmitted to the left ventricle during filling so that the left ventricular end-diastolic volume and pressure increase. Ventricular end-diastolic volume is also increased because in chronic mitral regurgitation the ventricle anatomically dilates (remodels) over years and decades. This increases the ventricular compliance. Increased end-diastolic volume would cause wall stress (afterload) to increase if it were not for the reduced outflow resistance and peak systolic pressure. The net effect of these changes is that the width of the pressure-volume loop is increased (i.e., ventricular stroke volume is increased); however, ejection into the aorta (forward flow) is reduced. The increased ventricular "stroke volume" (end-diastolic minus the end-systolic volume) in this case includes the volume of blood ejected into the aorta and the volume ejected back into the left atrium.
In chronic mitral regurgitation, systolic function becomes impaired, which leads to heart failure with reduced ejection fraction (HFrEF).
Revised 02/03/2024